Clinical & Hygienic Aspects of Exposure to Electromagnetic Fields.
Christopher Dodge, affiliated with the Library of Congress, wrote the first comprehensive review of the world (especially the Soviet and Eastern European) literature on the biological effects of microwaves in 1964. The current document was written 5 years later during which time the author was with the Biosciences Division, U.S. Naval Observatory, in Washington, D.C. This document concentrates on human clinical studies and occupational hygiene surveys of microwave exposure and is well worth reading.
What is clear is that by the late 1960 the Soviet and Eastern European scientists had conducted numerous studies on the effects of microwave radiation on humans, that biological and health effects were documented for a range of frequencies at non-thermal levels, and that this information was available to the U.S. military. Why this science was not taken more seriously, why guidelines were not influenced by this research, and why we are still debating thermal vs non-thermal effects is a mystery that I leave for historians and philosophers to debate.
Here are a few gems from this document:
- By 1933 Soviet scientists recognized that electromagnetic fields affected the human nervous system. Indeed changes to the central (CNS) and autonomic (ANS) nervous system attributed to radio frequency radiation were frequently documented, as were additional effects as shown in Table 1. Frequencies from 30 MHz to 300 GH at both thermal (greater than 10 mW/cm2) and non-thermal (microW/cm2 to milliW/cm2) intensities were known to affect the CNS.
- The most disappointing aspect of the literature cited was the absence of information on the specific circumstances of the irradiation, characteristics of the environment and the conditions of the body exposed, which makes repetition of the studies difficult.
- Panov et al. (1966) proposed three chronological stages of human response to microwaves (Table 2).
The first stage is not marked by severe episodes such as fainting or dramatic changes in pulse or blood pressure and the subject responds to outpatient treatment.
The second stage is called the “syndrome of autonomic and vascular dystonia” and the key features include altered pulse including bradycardia (slow) and tachycardia (rapid), either high or low blood pressure, altered ECG and general neuro-circulatory asthenia. Severe episodes (fainting) may occur and the subject requires hospitalization of unspecified nature or duration.
The third stage is called diencephalic syndrome in which visceral dysfunctions and crisis are observed. Typical episodes include apathic embolic disorders, hypersomnia, hypokinesis, hypothalamo-pituitary-suprarenal weakness, and inhibition of sexual and digestive reflexes. Panov claims these changes are not always reversible and that subjects require hospitalization. - The general subjective complaints resulting from EMR exposure shown in Table 3 resemble symptoms associated with electrohypersensitivity (EHS).
- Edelwejn (1966) found that the symptoms (Table 3) experienced by Polish personnel exposed to microwave radiation for up to six hours/day depended on the length of employment and degree of exposure. During the first three years, a dramatic response to microwave exposure accompanied by neurotic symptoms was reported. This was followed by a gradual adaption phase and then, many years later, by the reappearance of neurologic symptoms. Soviet workers exposed to electric and magnetic fields near hydroelectric stations also complained of symptoms in Table 3. Ospiov (1965) concluded that most subjective symptoms were reversible and that pathological damage to neural structures was insignificant.
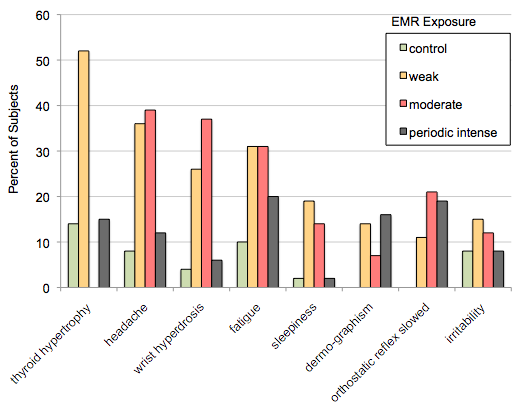
- In one study, a larger percentage of subjects exposed to weak (1 to 100s microW/cm2) and moderate (100s microW/cm2) levels of EMR experienced symptoms than those who were sporadically exposed to intense levels (3000 to 4000 microW/cm2) (see Figure 1 below, note this figure is based on Table 4 of the original document).
- Pulsed ultra high frequency (UHF) fields [0.3 to 3 GHz] could be used as a form of contactless electrosleep, which was called radio-sleep.
- Numerous changes were documented in the blood including altered blood sugar, cholesterol and lipids; altered levels of pyruvic acid, lactic acid, and creatinine; as well as hematopoietic [blood forming processes] and biochemical responses to electromagnetic radiation (see Tables 8,9, 10).
- Effects on the functioning of and damage to the eyes were mostly documented at either acute or chronic thermal levels of exposure (see Table 11).
- Major endocrine responses included altered functioning of the pituitary, thyroid and adrenal glands. Damage to sex glands and functions have been frequently documented after chronic exposure to primarily thermal intensities (Table 12). Decreased spermatogenesis, altered sex ratio at birth (excess females), changes in menstruation, retarded fetal development, congenital effects in newborns, decreased lactation in nursing mothers have been documented as result of thermal exposure (greater than 10,000 microW/cm2).

Figure 1. Percentage of subjects who responded to weak (1 to 100”²s microW/cm2), moderate (100”²s microW/cm2), and periodic intense (3,000 to 4,000 microW/cm2) levels of microwave radiation. Based on data in Table 4, Dodge, 1969. [Note: U.S. and Canadian guidelines are 1,000 microW/cm2 so the weak and moderate exposures are well below these guidelines.]