Dr. Weeks’ Comment: Again, once the consumer is not allowed to pay or even know the probable costs of a hospitalization, once it will all be taken care of by the third party, there is no accountability. As a medical student, I was shocked at how much was charged for hand held plastic urinals and how much was charged for the egg-crate mattress under the bed to soften the stay. Well, $546 for salt water! What do you think of them apples?
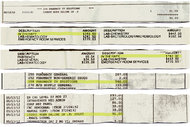
“…Dr. Frost, the anesthesiologist, spent three days in the same hospital and owed only $8, thanks to insurance coverage by United HealthCare. Still, she was baffled by the charges: $6,844, including $546 for six liters of saline that cost the hospital $5.16…”
How to Charge $546 for Six Liters of Saltwater
By NINA BERNSTEIN
Published: August 25, 2013
It is one of the most common components of emergency medicine: an intravenous bag of sterile saltwater.

Hospital bills for IV therapy vary wildly: $787 for an adult, $393 for a child at one hospital, and $546 for the saline, plus $127 for administering it, at another.
Podcast: Science Times
A food poisoning outbreak starts a reporter on an odyssey to find the price of saline solution; it turns out our existence may change the brains of the animals around us; a group of researchers is bringing water quality tracking to the taps we drink from.
Luckily for anyone who has ever needed an IV bag to replenish lost fluids or to receive medication, it is also one of the least expensive. The average manufacturer’s price, according to government data, has fluctuated in recent years from 44 cents to $1.
Yet there is nothing either cheap or simple about its ultimate cost, as I learned when I tried to trace the commercial path of IV bags from the factory to the veins of more than 100 patients struck by a May 2012 outbreak of food poisoning in upstate New York.
Some of the patients’ bills would later include markups of 100 to 200 times the manufacturer’s price, not counting separate charges for “IV administration.” And on other bills, a bundled charge for “IV therapy” was almost 1,000 times the official cost of the solution.
It is no secret that medical care in the United States is overpriced. But as the tale of the humble IV bag shows all too clearly, it is secrecy that helps keep prices high: hidden in the underbrush of transactions among multiple buyers and sellers, and in the hieroglyphics of hospital bills.
At every step from manufacturer to patient, there are confidential deals among the major players, including drug companies, purchasing organizations and distributors, and insurers. These deals so obscure prices and profits that even participants cannot say what the simplest component of care actually costs, let alone what it should cost.
And that leaves taxpayers and patients alike with an inflated bottom line and little or no way to challenge it.
A Price in Flux
In the food-poisoning case, some of the stricken were affluent, and others barely made ends meet. Some had private insurance; some were covered by government programs like Medicare and Medicaid; and some were uninsured.
In the end, those factors strongly (and sometimes perversely) affected overall charges for treatment, including how much patients were expected to pay out of pocket. But at the beginning, there was the cost of an IV bag of normal saline, one of more than a billion units used in the United States each year.
“People are shocked when they hear that a bag of saline solution costs far less than their cup of coffee in the morning,” said Deborah Spak, a spokeswoman for Baxter International, one of three global pharmaceutical companies that make nearly all the IV solutions used in the United States.
It was a rare unguarded comment. Ms. Spak ”” like a spokesman for Hospira, another giant in the field ”” later insisted that all information about saline solution prices was private.
In fact, manufacturers are required to report such prices annually to the federal government, which bases Medicare payments on the average national price plus 6 percent. The limit for one liter of normal saline (a little more than a quart) went to $1.07 this year from 46 cents in 2010, an increase manufacturers linked to the cost of raw materials, fuel and transportation. That would seem to make it the rare medical item that is cheaper in the United States than in France, where the price at a typical hospital in Paris last year was 3.62 euros, or $4.73.
Middlemen at the Fore
One-liter IV bags normally contain nine grams of salt, less than two teaspoons. Much of it comes from a major Morton Salt operation in Rittman, Ohio, which uses a subterranean salt deposit formed millions of years ago. The water is local to places like Round Lake, Ill., or Rocky Mount, N.C., where Baxter and Hospira, respectively, run their biggest automated production plants under sterility standards set by the Food and Drug Administration.
But even before the finished product is sold by the case or the truckload, the real cost of a bag of normal saline, like the true cost of medical supplies from gauze to heart implants, disappears into an opaque realm of byzantine contracts, confidential rebates and fees that would be considered illegal kickbacks in many other industries.
IV bags can function like cheap milk and eggs in a high-priced grocery store, or like the one-cent cellphone locked into an expensive service contract. They serve as loss leaders in exclusive contracts with “preferred manufacturers” that bundle together expensive drugs and basics, or throw in “free” medical equipment with costly consequences.
Few hospitals negotiate these deals themselves. Instead, they rely on two formidable sets of middlemen: a few giant group-purchasing organizations that negotiate high-volume contracts, and a few giant distributors that buy and store medical supplies and deliver them to hospitals.
Proponents of this system say it saves hospitals billions in economies of scale. Critics say the middlemen not only take their cut, but they have a strong interest in keeping most prices high and competition minimal.
The top three group-purchasing organizations now handle contracts for more than half of all institutional medical supplies sold in the United States, including the IVs used in the food-poisoning case, which were bought and taken by truck to regional warehouses by big distributors.
These contracts proved to be another black box. Debbie Mitchell, a spokeswoman for Cardinal Health, one of the three largest distributors, said she could not discuss costs or prices under “disclosure rules relative to our investor relations.”
Distributors match different confidential prices for the same product with each hospital’s contract, she said, and sell information on the buyers back to manufacturers.
A huge Cardinal distribution center is in Montgomery, N.Y. ”” only 30 miles, as it happens, from the landscaped grounds of the Buddhist monastery in Carmel, N.Y., where many of the food-poisoning victims fell ill on Mother’s Day 2012.
Among them were families on 10 tour buses that had left Chinatown in Manhattan that morning to watch dragon dances at the monastery. After eating lunch from food stalls there, some traveled on to the designer outlet stores at Woodbury Common, about 30 miles away, before falling sick.
The symptoms were vicious. “Within two hours of eating that rice that I had bought, I was lying on the ground barely conscious,” said Dr. Elizabeth Frost, 73, an anesthesiologist from Purchase in Westchester County who was visiting the monastery gardens with two friends. “I can’t believe no one died.”
About 100 people were taken to hospitals in the region by ambulance; five were admitted and the rest released the same day. The New York State Department of Health later found the cause was a common bacterium, Staphylococcus aureus, from improperly cooked or stored food sold in the stalls.
Mysterious Charges
The sick entered a health care ecosystem under strain, swept by consolidation and past efforts at cost containment.
For more than a decade, hospitals in the Hudson Valley, like those across the country, have scrambled for mergers and alliances to offset economic pressures from all sides. The five hospitals where most of the victims were treated are all part of merged entities jockeying for bargaining power and market share ”” or worrying that other players will leave them struggling to survive.
The Affordable Care Act encourages these developments as it drives toward a reimbursement system that strives to keep people out of hospitals through more coordinated, cost-efficient care paid on the basis of results, not services. But the billing mysteries in the food poisoning case show how easily cost-cutting can turn into cost-shifting.
A Chinese-American toddler from Brooklyn and her 56-year-old grandmother, treated and released within hours from the emergency room at St. Luke’s Cornwall Hospital, ran up charges of more than $4,000 and were billed for $1,400 ”” the hospital’s rate for the uninsured, even though the family is covered by a health maintenance organization under Medicaid, the federal-state program for poor people.
The charges included “IV therapy,” billed at $787 for the adult and $393 for the child, which suggests that the difference in the amount of saline infused, typically less than a liter, could alone account for several hundred dollars.
Tricia O’Malley, a spokeswoman for the hospital, would not disclose the price it pays per IV bag or break down the therapy charge, which she called the hospital’s “private pay rate,” or the sticker price charged to people without insurance. She said she could not explain why patients covered by Medicaid were billed at all.
Eventually the head of the family, an electrician’s helper who speaks little English, complained to HealthFirst, the Medicaid H.M.O. It paid $119 to settle the grandmother’s $2,168 bill, without specifying how much of the payment was for the IV. It paid $66.50 to the doctor, who had billed $606.
At White Plains Hospital, a patient with private insurance from Aetna was charged $91 for one unit of Hospira IV that cost the hospital 86 cents, according to a hospital spokeswoman, Eliza O’Neill.
Ms. O’Neill defended the markup as “consistent with industry standards.” She said it reflected “not only the cost of the solution but a variety of related services and processes,” like procurement, biomedical handling and storage, apparently not included in a charge of $127 for administering the IV and $893 for emergency-room services.
The patient, a financial services professional in her 50s, ended up paying $100 for her visit. “Honestly, I don’t understand the system at all,” said the woman, who shared the information on the condition that she not be named.
Dr. Frost, the anesthesiologist, spent three days in the same hospital and owed only $8, thanks to insurance coverage by United HealthCare. Still, she was baffled by the charges: $6,844, including $546 for six liters of saline that cost the hospital $5.16.
“It’s just absolutely absurd.” she said. “That’s saltwater.”
Last fall, I appealed to the New York State Department of Health for help in mapping the charges for rehydrating patients in the food poisoning episode. Deploying software normally used to detect Medicaid fraud, a team compiled a chart of what Medicaid and Medicare were billed in six of the cases.
But the department has yet to release the chart. It is under indefinite review, Bill Schwarz, a department spokesman, said, “to ensure confidential information is not compromised.”
This article has been revised to reflect the following correction:
Correction: August 29, 2013
An article on Tuesday about the cost of an intravenous bag of sterile saltwater misstated part of the name of a group of designer outlet stores in Central Valley, N.Y., which some victims of a food poisoning outbreak visited after eating lunch from food stalls at a Buddhist monastery in Carmel, N.Y., in May 2012. It is Woodbury Common (not Commons).